These days, we hardly ever think about bridges. I mean proper ones that you drive cars over.
Yet in the late 1800's and early 1900's, especially in the vast development of the American west, steel bridges collapsed at a terrific rate.
Steel was this amazing new technology for bridge building and it allowed these incredibly delicate, long, aesthetic designs to be built at low cost.
From that time, obviously engineering got a lot better and the ability of engineers to calculate how bridges worked, or didn't got better.
But it is also true to say that most bridges now have a factor of safety built into them. Or more simply, over-engineering.
Over-engineering is always in tension with Value Engineering.
One is focussed in never going wrong. The other is focused on giving the best utility for a given monetary amount.
This tension is also slugging it out every day in dentistry and as yet, no winner has been declared. And nor will ever be.
In general, factor of safety will be increased as something gets more important.
A landmark bridge will often be designed with a higher factor of safety than perhaps a creek crossing in the middle of a city. This is because it's safety is much more crucial and it's more difficult to build in the first place.
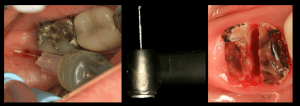
Implants are one of the areas where we most commonly build complex bridges in dentistry where we have a lot of control over the engineering and see this tension between safety and value.
On one hand, you have the value folks. All on four. All on three. Some even claim all on two! (I do all none sometimes). What is interesting is that often less implantitis now claimed to be ideal on some oral hygiene basis despite having no long term data that this improves success. This may be more PR than anything.
The other are the Branemark/Misch folks who like all on eight/six.
I've noticed a consistent theme here.
When I read old, long term papers by Branemark, they show a thing called bone resorption. And often random implants will show severe bone loss (now we would call this peri-implantitis).
When I see thirty year old cases from Ady Palti, They have bone loss. Threads out. Often a single implant failing. But because there are six or eight implants, the case is still surviving despite losing an implant or two.
When I see lectures by Howie Gluckman or Robert Oretti, people with a lot of long term cases, they talk about bone resorption. Tissue thinning. Peri-implantitis as cases get older.
There is so much talk about how to solve bone resorption. Non-resorbing cow bone. Socket shield. Overbuilding. Soft tissue grafts. All of these have shown excellent long term results for at least two years now. :))
So far, I'm pessimistic that we can change biology.
So how to decide?
Should we over-engineer dentistry and make it out of reach of many? Or should we value engineer and risk total failure from this pernicious loss of bone that has been going on forever?
I don't know the answer.
Like road bridges, the more catastrophic a failures is, the more you should consider over-engineering (putting extra implants).
For me, I ask the patient. I feel if they can only just afford a value engineered job, they may not be able to afford any failure, complication or disaster.
And when the patient cannot afford to pay for problems, there is a very high risk that we will end up paying for it.
You can perhaps get around this with a very lengthy legal document. But when you need a legal document to get away with value engineering, it perhaps tells you that it's not a good idea. What are your thoughts?